The number one cause of spinal fractures is trauma from high-impact injuries such as car accidents, a long fall, a sports accident, or a gunshot wound. These high-impact injuries require emergency treatment. Other spinal fractures may result from a low-impact injury from a minor fall or from bone insufficiency caused by osteoporosis, tumors, or other underlying conditions that weaken the bone. Over time, spinal fractures from bony insufficiency may develop unnoticed with no symptoms or discomfort until a bone breaks.
In osteoporosis, the bones become brittle and weak, making them susceptible to fractures even from simple bending or coughing.
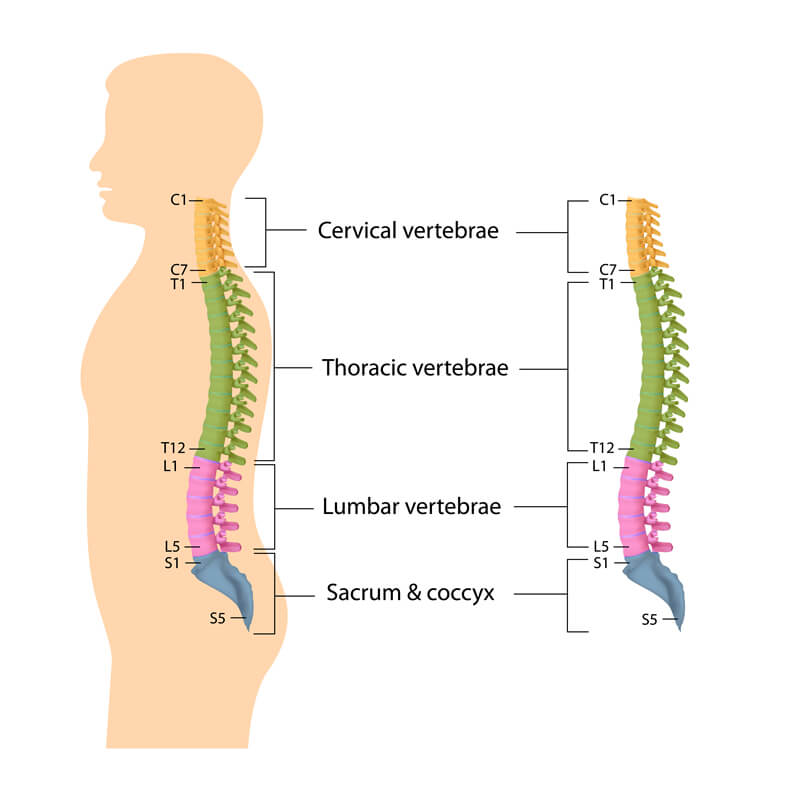
Spine Anatomy
The vertebral column usually consists of 33 vertebrae, 24 presacral vertebrae (seven cervical, 12 thoracic, and five lumbar), followed by the sacrum (five fused sacral vertebrae), and the coccyx (four frequently fused coccygeal vertebrae).
Most spinal fractures occur in the midback (thoracic spine) and the low-back (lumbar spine). Treatment often depends on the severity of the fracture and whether the patient has other injuries affecting the spinal cord and/or nerve function.
Types of Spinal Fractures
There are three different types of spine fractures. Dr. Ball will classify the fracture of the thoracic and/or lumbar spine based on the fracture’s specific pattern and whether there is a spinal cord injury. Classifying the fracture pattern helps to determine the proper treatment.
The three major types of spine fracture patterns are
Flexion Fracture Pattern. A flexion fracture pattern can be either a compression fracture or an axial burst fracture. In a compression fracture, the front (anterior) of the vertebra breaks and loses height, but the back (posterior) vertebra does not. These fractures are usually stable fractures, meaning the bones have not moved out of place, and they are rarely associated with neurologic problems. Compression fractures commonly occur in patients with osteoporosis.
In an axial burst fracture, the vertebra loses height on both the front and back sides. It is often caused by landing on the feet after falling from a significant height. These fractures may sometimes result in nerve compression, and they can be either stable or unstable (the bones have moved out of place) fractures.
Extension Fracture Pattern. In an extension fracture pattern or flexion/distraction (Chance) fracture, the vertebra is pulled apart (distraction). This type of fracture can occur in a head-on car collision when the upper body is thrown forward while a lap seat belt stabilizes the pelvis. Typically, these are unstable fractures.
Rotation Fracture Pattern. A rotation fracture pattern can be either a transverse process fracture or a fracture-dislocation. In a transverse process fracture, which is uncommon, the fracture results from rotation or extreme sideways (lateral) bending. Usually, these fractures do not affect stability.
In a fracture-dislocation, there is a fracture and dislocation of the vertebrae. These fractures are unstable, and frequently they cause serious spinal cord compression and injury, often permanent.
Symptoms of Spinal Fractures
The main symptom of a spinal fracture of the thoracic or lumbar spine is moderate to severe back pain that worsens with movement.
If the spinal cord or nerves are involved, symptoms may also include bowel/bladder dysfunction along with numbness, tingling, or weakness in the limbs.
If the spinal fracture is due to a high-impact injury from a car accident, for example, a patient may have a brain injury as well and lose consciousness.
Emergency Treatment for Suspected Spinal Fractures
High-impact trauma injuries suspect of thoracic or lumbar spinal fractures require emergency treatment at the accident site. EMS rescue workers will check the patient’s vital signs, including consciousness, ability to breathe, and heart rate. Once stabilized, the rescue workers will assess obvious bleeding and limb-deforming injuries.
Before moving the patient, the EMS team will immobilize the patient in a cervical (neck) collar and backboard.
Emergency Room Evaluation for Suspected Spinal Fractures
Once at the hospital, the trauma team will complete and thoroughly evaluate the head, chest, abdomen, pelvis, limbs, and spine. The emergency doctor will assess the patient’s neurological status, including testing his or her ability to move, feel, and sense the position of all the limbs. Reflexes will also be tested to determine if there is an injury to the spinal cord or individual nerves. The tone of the anal muscles will be tested to determine if the patient is able to empty his or her bladder without assistance. Problems with bowel and bladder functions may indicate a more serious spinal cord injury.
Diagnosing Spinal Fractures
Depending on the extent of the injury, Imaging tests such as X-rays, CT scans, or MRI scans of the thoracic and lumbar spine may be ordered.
Treatment for Spinal Fractures
Stable fractures that do not compromise spinal cord or nerve function may be treated nonsurgically with immobilization or bracing for 6 to 12 weeks, while unstable high-energy fractures or those with neurological compromise need to be treated surgically on an urgent basis.
If spinal surgery is needed for a spinal fracture, the goals are to achieve adequate reduction (return the bones to their proper position), stabilize the fracture, relieve pressure on the spinal cord and nerves, and allow for early movement. Metal screws, rods, and cages are used to stabilize the spine.
Recovery After Spinal Fracture Treatment
After a fracture has healed, there will be a period of rehabilitation. The goal of rehabilitation is to reduce pain, restore mobility, and return the patient to his/her preinjury state (as much as possible). Physical therapy is recommended for patients to help them reach these goals.
Patients who had spinal fractures due to osteoporosis are at an increased risk for additional fractures, so Dr. Ball may recommend additional treatments to address bone density loss. For these patients, other treatments, such as kyphoplasty, may be recommended. Kyphoplasty is a minimally invasive procedure used to treat vertebral compression fractures by inflating a balloon to restore bone height then injecting bone cement into the vertebral body.
Spinal Fracture Treatment at CalSpine MD
If you have sustained a spinal fracture from a high-impact injury or the result of osteoporosis, contact CalSpine MD at (925) 667-3565 to schedule an appointment for spinal fracture treatment. You may also Request An Appointment online.